 |
| Image Credit: Wikimedia |
{kind=link}
 |
| This post was peer reviewed. Click to learn more. |
Author: Bill Christian, MS-4
Ross University School of Medicine
AAEM/RSA Publications and Social Media Committee
Rapid assessment of the left ventricular ejection fraction (LVEF) may be critical for the emergency physician. Imagine a patient comes into your emergency department (ED) with acute dyspnea. He has a history of congestive heart failure, chronic obstructive pulmonary disease and myocardial infarction. Can ultrasound help differentiate between some of the many potential causes of dyspnea? Yes!
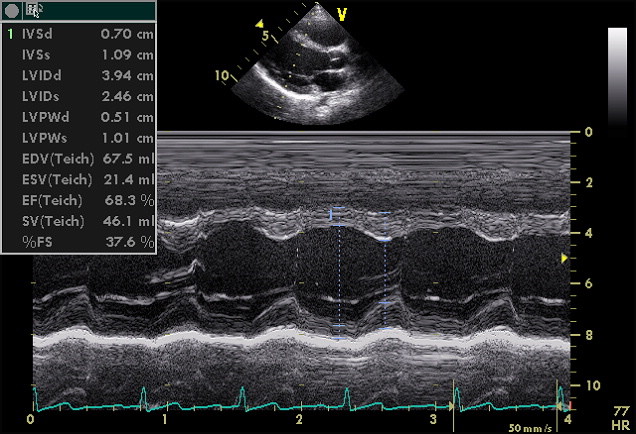
One rapid technique to assess the LVEF can be done using the mitral valve. Normally, the anterior mitral valve leaflet should approach or touch the septum. However, in systolic heart failure, the ballooning heart with increased preload will pull the valve away from the septum. In early diastole, the anterior mitral valve reaches a point of maximum excursion and comes closest to the ventricular septum, which is called the E-point. Measuring the distance between the anterior mitral valve and the ventricular septum in early diastole is called the E-point septal separation (EPSS)(see Figure 1). Once obtained, the EPSS can be plugged into a formula for a quick estimation of LVEF.
 |
| Figure 1. M-mode at Anterior Mitral Valve. E = E point. EPSS = E-Point Septal Separation. IVS = Interventricular Septum. |
{kind=link}
In order to obtain the EPSS, first ensure the patient is in a supine position. Position the probe in the parasternal long axis view. Use the M-mode to place the marker over the most distal tip of the anterior mitral valve as shown in blue. Identify the E point (yellow) and interventricular septum (green) and measure between those two points (red).
Once the EPSS is obtained, how does one interpret it? One fast method is to have a cutoff of 7 mm in mind. One study showed the EPSS measurement of 7 mm or greater was 100% sensitive and 51.6% specific for severely reduced LVEF, along with a positive likelihood ratio of 2.07.[1] In addition, the EPSS measurement may be inserted into a formula[2]: LVEF = 75.5 - (2.5 x EPSS). For a rapid assessment of LVEF, think of 7mm and under!
As with many diagnostic tests, there are limitations and results must be interpreted in an appropriate context. For example, aortic regurgitation and mitral stenosis can falsely elevate EPSS, as both cause an abnormally increased distance between the mitral valve and septum during early diastole.[3] In addition, one must have the base knowledge to properly differentiate the E-point and interventricular septum for proper measurement. However, when applied correctly, even less experienced emergency physicians can obtain LVEF estimates that correlate closely with visual estimates of clinicians with extensive echocardiography experience.[4] Just keep in mind the context of your patient’s history while interpreting the EPSS measurement.
Knowing how to measure the EPSS is a simple and easy tool to have when estimating LVEF, as it only requires the use of the parasternal long axis view and M-mode. As always, be cautious of interpretation and aware of mitral pathologies. This mitral valve measurement method can potentially complement and strengthen your assessment.
References:
1. Mckaigney CJ, Krantz MJ, Rocque CLL, Hurst ND, Buchanan MS, Kendall JL. E-point septal separation: a bedside tool for emergency physician assessment of left ventricular ejection fraction. Am J Emerg Med. 2014;32(6):493-497. doi:10.1016/j.ajem.2014.01.045.
2. Silverstein JR, Laffely NH, Rifkin RD. Quantitative estimation of left ventricular ejection fraction from mitral valve E-point to septal separation and comparison to magnetic resonance imaging. Am J Cardiol. 2006;97(1):137-140. doi:10.1016/j.amjcard.2005.07.118.
3. Ahmadpour H, Shah AA, Allen JW, Edmiston W, Kim SJ, Haywood L. Mitral E point septal separation: a reliable index of left ventricular performance in coronary artery disease. Am Heart J. 1983;106(1):21-28. doi:10.1016/0002-8703(83)90433-7.
4. Secko MA, Lazar JM, Salciccioli LA, Stone MB. Can junior emergency physicians use E-point septal separation to accurately estimate left ventricular function in acutely dyspneic patients? Acad Emerg Med. 2011;18(11):1223-1226. doi:10.1111/j.1553-2712.2011.01196.x.
No comments:
Post a Comment